Evaluation of the Usefulness of 2D MultiVane XD iMSDE in Enhanced T1 Weighted Carotid Vessel Wall Imaging: Comparison with 3D TSE iMSDE
분당서울대학교병원 영상의학과1 2 3 4
Department of Radiology, Seoul National University Bundang Hospital1 2 3 4
교신저자: 정재윤, 분당서울대학교병원 영상의학과, Tel: 031-787-2862, Fax: 031-787-4011, e-mail: 20352@snubh.org
Corresponding author: Jae-Yun Jeong, Department of Radiology, Seoul National University Bundang Hospital, Tel: 031-787-2862, Fax: 031-787-4011, e-mail: 20352@snubh.org
취약하다. 이러한 움직임들을 보정하기 위해 본 연구는 2D MVXD iMSDE와 기존의 3D TSE iMSDE를 비교하여 그
유용성을 평가 하고자 하였다. 2017년 2월부터 7월까지 내원한 carotid vessel wall MRI 검사 환자 30명(남: 16, 여:
14, 평균연령: 62.5±10.39 years)을 대상으로 하였다. 사용된 장비는 3.0T Ingenia CX이며 32 channel sense head
coil을 사용하였다. Pulse sequence는 2D MVXD iMSDE와 3D TSE iMSDE 두 기법이며 각각 조영증강 후 지방 소
거 T1강조영상을 적용 하였다. 검사 시간은 각각 4분06초, 2분55초였다. 획득된 영상의 상대적 대조도 비(relative
contrast ratio)를 구하기 위해, 두 기법의 좌, 우 common carotid artery bifurcation지점의 혈관 벽과 내강의 신호강도
(signal intensity)를 3회 측정하여 평균값을 구하였고, 각 영상들의 motion artifact정도, blood suppression정도, image
sharpness정도에 대해 MRI 전문방사선사 4명이 리커트 척도(1= unacceptable, 2= poor, 3= normal, 4= good, 5=
very good)로 정성적 평가를 하였다. 두 기법의 RCR평균값 측정결과 2D MVXD iMSDE 는 Rt에서 8.75±1.68, Lt
에서 8.91±2.43, 3D TSE iMSDE는 Rt에서 8.92±1.72, Lt에서 9.11±1.73로 3D TSE iMSDE에서 RCR평균값이
더 높았고 통계학적 분석결과 유의한 차이를 보이지 않았다. 정성적 평가에서 blood suppression, image sharpness항
목은 비슷하였으나 motion artifact항목에서는 2D MVXD iMSDE가 더 높게 평가 되었다. 통계학적 분석결과 motion
artifact 항목만 유의한 차이를 보였고, 다른 두 항목에서는 유의한 차이를 보이지 않았다. 따라서, 움직임으로 인해
motion artifact가 발생하는 환자에게는 2D MVXD iMSDE를 사용하는 것이 보다 진단적 가치 있는 영상을 획득 하는
데 유용할 것이라 사료된다.
movements (breathing, swallowing, and coughing). To compensate for these movements, this
study evaluates the usefulness of 2D Multi Vane XD iMSDE compared with 3D TSE iMSDE.
Thirty patients who visited Seoul National University Bundang Hospital for carotid vessel
wall examination from February to July in 2017 were enrolled in this study (male: 16 female:
14; mean age: 62.5±10.39 years). The equipment 3.0T Ingenia CX and 32-channel head coil
were used for image acquisition. We obtained fat saturated T1-weighted axial images of 2D
MVXD iMSDE and 3D TSE iMSDE after injection of contrast media on both carotid artery
bifurcation levels. The scan time was 4m06sec and 2m55sec respectively. To measure the
Relative-Contrast-Ratio of the acquired images, signal intensity of the both bifurcation levels
were obtained by measuring three-times and averaged on lumen and vessel wall. Qualitative
assessment was performed regarding each images degree of motion artifact, degree of blood
suppression, image sharpness, using Likert 5 scale(1= unacceptable, 2= poor, 3= normal, 4=
good, 5= very good) by five radiologic technologists with more than five years of experience.
Results of the RCR average of both techniques, 2D MVXD iMSDE was 8.75±1.68at the Rt,
8.91±2.43at the Lt, and 3D TSE iMSDE was 8.92±1.72 at the Rt, 9.11±1.73at the Lt. Even
though the RCR average was higher in 3D TSE iMSDE, there is no significant difference
between 2D MVXD iMSDE and 3D TSE iMSDE in statistical analysis result. In the qualitative
assessment, both techniques were similar in blood suppression and image sharpness. However
2D MVXD iMSDE was higher assessment than 3D TSE iMSDE in motion artifact. The
statistical analysis result, motion artifact showed significant difference but the others have no
significant differences. Therefore, it is recommended to use 2D MVXD iMSDE for patients
who motion artifact occurred by severe motion.
2015년 통계청에서 보고한 사망원인통계 자료에 따르면 대한민국 사망원인 중 뇌혈관질환으로 인한 사망률은
암, 심장 질환에 이어 3위를 차지하고 있으며, 인구 10만명당 48명이 뇌혈관 질환으로 사망하였다고 보고되었다.
뇌혈관 질환에 관련된 혈관 중, 경동맥은 뇌로 가는 혈액의 약 80%를 공급하는 혈관으로 경동맥 질환은 대부분
죽상동맥경화증에 의해 발생한다. 허혈성 뇌졸중 환자 중 약 20%가 이 경동맥 죽상동맥경화증이 원인이며
경동맥이 죽상경화반으로 협착되어 막히거나, 협착이 심하지 않더라도 취약판의 표면이 손상되어 혈전이 떨어져 나가면
혈관을 막으면서 뇌경색이 발생 할 수 있다.
경동맥은 임상적으로 죽상동맥경화증이 호발하는 부위이며 내강의 이상뿐만 아니라 혈관 벽의 기하학적, 형태학적 평가가
매우 중요하다. 경동맥 내 죽상경화반과 혈관 벽을 진단하는 방법으로는 혈관조영술, 전산화 단층촬영(CT), 초음파(US),
자기공명영상(MRI) 등이 있다. 이중 혈관조영술은 혈관의 형태를 파악하기에는 우수하지만 환자에게 침습적이고
혈관 벽의 구조나 성질을 평가하기 어려우며 전산화 단층촬영은 혈관 내 석회화 병변을 구분해내는 데는 우수하나
미세한 hemorrhage, necrotic lipid core등을 구분하는 데는 제한적이다. 초음파는 내경동맥과 분지 부위의 혈관내막
두께 측정이 어렵고 soft plaque의 정확한 정보제공에 제한이 있다. 이에 비해 자기공명영상은 검사 시간은 길지만
비침습적이고 혈관의 두께와 협착 정도 및 plaque의 주요 구성성분을 비교적 정확하게 구분해 낼 수 있으며
치료 경과를 평가 할 수 있다.
자기공명영상을 통한 plaque 진단 기법 중 하나인 black blood 기법은 혈관 벽과 내강의 경계를 식별하고
혈관 벽의 해부학적 구조와 질병을 평가하는 데 이용된다. 혈관 벽과 내강에 대한 정확한 형태와 진단을 위해서는
효율적인 혈류 신호의 억제가 매우 중요하다.
그러나 경동맥 분지 지점에서는 복잡한 혈류 패턴(slow and turbulent flow)으로 인해 black blood 기법에서
plaque처럼 보이는 artifact가 자주 발생하며 이로 인해 혈관 벽의 형태와 plaque 크기가 부정확하게 측정 될 수 있다.
이에 최근에는 효율적인 혈류 신호의 억제를 위해 3D Turbo spin echo (TSE)와 함께 improved motion sensitized
driven equilibrium (iMSDE)를 이용한 black blood 기법이 사용되고 있다.
Turbo spin echo는 불균질한 자기장에 덜 민감하고 T1, T2, 양성자 밀도 강조영상 등을 이용하여 여러 조직의 대조도를
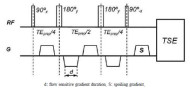
우수하게 나타내기 때문에 black blood 기법에서 우선적으로 사용된다. iMSDE는 기존의 MSDE기법에 추가적으로
180° 재자화 펄스를 더하여 MSDE기법에서의 eddy current와 B1 inhomogeneity로 인한 신호 소실을 보상해준다(Fig. 1).
3D TSE iMSDE black blood image는 우수한 해상력과 CNR로 혈관 벽과 죽상동맥경화반을 영상화 하지만
경동맥의 해부학적 위치 특성상 환자의 침 삼킴, 호흡, 기침 등에 의한 motion artifact에 취약하다.
이는 기존의 2D image와 비교하여 검사 시간이 길고 검사 중 발생하는 motion이 영상 전체 dataset에 영향을 미치기 때문이다.
이러한 motion artifact를 극복하기 위해 개발된 MultiVane (philips healthcare, netherlands) 기법은 변형된 TSE 기법으로
motion artifact가 적은 영상을 제공한다. MultiVane기법에서 한번의 TR동안 k-space의 중심을 통과하는 직사각형 모양의
다중병렬 위상부호화 줄(multiple parallel phase-encoded line)들을 vane이라 하며 각각의 vane들은 k-space 중심을 축으로
회전하며 sampling한다. 그 결과 k-space sampling 패턴은 propeller 모양처럼 되며 k-space의 중심부는
각각의 vane들로부터 중첩되어 oversample 된다. MultiVane기법은 각각의 vane들의 비교를 통해 환자의 inplane motion을
수정하고 손상된 데이터의 vane을 식별하여 최종 재구성 작업에서 제외시킨다.
그러므로 MultiVane기법은 기존의 TSE 기법에 비해 motion에 덜 민감하다.
하지만 MultiVane의 data 획득시간은 k-space 중심부의 oversampling으로 인해 기존의 TSE기법보다 최소 50% 더 길다는
제한점이 있었다17(Fig. 2).
최근에는 이러한 제한점을 극복하기 위해 기존의 Multi Vane 기법에 병렬영상 기법 (parallel imaging)을 적용 시켜
검사 시간을 획기적으로 줄 일수 있는 MultiVane XD(이하 MVXD) 기법이 개발 되었다.
이에 본 연구는 carotid vessel wall 검사 시 flow artifact를 보다 더 효과적으로 suppression 할 수 있는 iMSDE기법과
환자의 motion artifact를 보정할 수 있는 MVXD기법을 접목시킨 2D MVXD iMSDE기법을 3D TSE iMSDE기법과 비교하여
그 유용성을 평가하고자 하였다.
2.1 기간 및 연구 대상
본 연구는 2017년 2월 1일부터 7월 31일까지 본원을 내원하여 carotid vessel wall MRI를 시행한 환자들을
대상으로 하였다. 성별은 남성 16명, 여성 14명이고 평균연령은 62.5±10.39세였다.
2.2 장비 및 검사 방법
연구에 사용된 장비는 Ingenia CX 3.0T (Philips, Netherland)이고, 코일은 32channel sense head coil을 사용하였다.
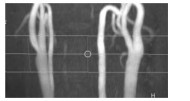
검사 부위는 좌, 우 carotid artery의 bifurcation을 중심으로 축상 면 영상을 획득하였다(Fig. 3).
동일 환자에게 2D MultiVane XD iMSDE와 3D TSE iMSDE를 적용하였고 두 기법 모두 조영증강 후 지방소거 T1강조영상으로
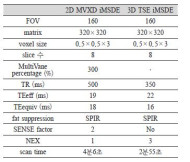
획득하였다. 사용된 매개변수는 Table 1과 같다(Table 1).
2.3 영상 분석 방법
2.3.1 정량적 평가
두 영상의 좌우 distal common carotid artery bifurcation지점에서 내강과 혈관 벽 부위에 각각10 mm2, 1mm의 관심영역
(region of interest)을 설정하여 신호강도(signal intensity: SI)를 3회 측정하였고, 두 관심영역(wall, lumen)의
상대적 대조도 비(relative contrast ratio, RCR)를 계산한 뒤 평균값을 측정하였다(Eq. 1).
이때 혈관 벽의 신호강도는 S1, S2, S3, S4 4개의 위치에서 측정 후 평균값으로 계산하였다(Fig. 4).
각각의 영상에서 측정된 RCR값에 대한 통계학적 분석은 대응표본 T검정(SPSS 18.0K for windows)을 이용하였으며,
p값이 0.05미만일 경우 유의한 것으로 판단하였다.
RCR = [(S1+S2+S3+S4)/4] / lumen SI ------ (Eq. 1)
2.3.2 정성적 평가
두 기법에 의해 획득한 영상을 임상경력 5년 이상의 MRI전문방사선사 4명이 리커트 척도(1점= unacceptable,2점= poor,
3점= normal, 4점= good, 5점= very good)로 점수화 하여 평가하였다.
평가 항목으로는 motion artifact정도, blood suppression정도, image sharpness정도를 평가하였으며
각 항목 당 점수를 합하여 평균 내었다. 평균 낸 값은 대응표본 T 검정(SPSS18.0K for windows)를 사용하
p값이 0.05미만일 경우 통계적으로 유의한 것으로 판단하였다.
3.1 정량적 평가
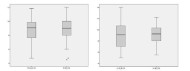
각 관심영역의 signal intensity 측정 후 RCR을 비교 분석한 결과, 2D MVXD iMSDE에서 Rt의 평균값은 8.75±1.68,
Lt의 평균값은 8.91±2.43으로 측정되었고, 3D TSE iMSDE에서 Rt의 평균값은 8.92±1.72,
Lt의 평균값은 9.11±1.73로 측정되었다(Fig. 5). 대응표본 T 검정을 통한 통계 분석 결과 유의한 차이를 보이지 않았다 (p>0.05) (Table 2).
3.2 정성적 평가
3가지 항목의 정성적 평가 결과, 2D MVXD iMSDE에서 motion artifact 4.37, blood suppression 3.92,
image sharpness 4.07로 평가되었다. 3D TSE iMSDE의 경우 motion artifact 3.54, blood suppression 3.88,
image sharpness 3.8로 평가되었으며 모든 항목에서 2D MVXD iMSDE가 높게 측정되었다.
통계 분석 결과 motion artifact 항목에서는 p<0.05 (p=0)로 유의한 차이를 보였고 blood suppression 항목과
image sharpness항목에서는 p>0.05로 유의한 차이를 보이지 않았다(Table 3).
Carotid vessel wall 검사 시, 3D TSE는 3D의 향상된 해상력과 함께 TSE의 T1, T2, 양성자 밀도 강조영상 등을
이용하여 plaque의 형태와 구성성분을 감별한다. 여기에 iMSDE의 병행은 flow의 효과적인 suppression까지되어
현재 임상에서 보편적으로 사용하고 있는 기법이 되었다. 하지만 carotid artery의 해부학적 위치 특성상 많은 검사에서
환자의 motion(삼킴, 호흡, 기침 등)으로 인한 artifact가 발생하였고 이는 영상의 질을 저하시키는 주된 원인이 되었다.
이러한 문제점들을 극복하기 위해 기존의 black blood기법과 비교하여 그 유용성을 검증하기 위한 많은 연구들이 이루어졌다.
Lindsey A. Crowe19 등은 3D TSE DIR (double inversion recovery)에 navigator를 적용하는 기법을 연구하였고
실험 결과, navigator로 인해 motion artifact는 감소하였다. 하지만 부정맥 환자나 swallowing시 heart rate의 상승은
DIR기법에 영향을 미쳐 blood suppression 효과를 감소시켰다. Masami Yoneyama20등은 hyperecho MultiVane기법을
연구하였고 그 결과, motion artifact감소와 blood suppression정도에 모두 효과적이었다.
하지만 hyperecho의 특성상 증가하는 echo train length (ETL)로 인해 유효TE (TEeff)값이 증가하였고 이는 T2강조영상에만
적용할 수 밖에 없는 한계가 있었다.
본 연구는 앞서 두 연구의 제한점을 보완하고자 2D multi vane XD 기법에 iMSDE기법을 병행하였고 조영증강 후 지방소거
T1강조영상을 이용하여 비교 분석하였다. 이는 조영증강 전 T1강조영상보다 증강 후 T1 강조영상에서 보다 확실한
plaque의 감별이 이루어지기 때문이다.
연구 결과, 정량적 평가에서 3D TSE iMSDE가 2D MVXD iMSDE보다 좌∙우 측 모두 RCR 평균값이 조금 높게 측정 되었고
통계적으로 유의한 차이는 없었다. 정성적 평가결과, 두 기법에서 blood suppression과 image sharpness항목은
2D MVXD iMSDE가 조금 더 높은 평가를 받았으나 통계적으로 유의한 차이는 없었다.
그러나 motion artifact 항목에서는 2D MVXD iMSDE가 3D TSE iMSDE보다 더 높은 평가를 받았으며 통계적으로
유의한 차이를 보였다(Fig. 6). 즉, RCR과 blood suppression 정도, image sharpness면에서는 두 기법간 큰 차이가
없음을 알 수 있었고 motion artifact정도에서는 2D MVXD iMSDE가 유용 한 것을 확인할 수 있었다.
하지만 2D와 3D간의 기법 차이와 multi vane의 radial 방식, 3D TSE의 cartesian방식의 k-space data 획득방법 차이로 인
SNR과 CNR의 정량적 비교 평가가 어려운 점이 아쉬움으로 남는다.
결론적으로 움직임으로 인해 motion artifact가 발생하는 환자에게는 3D iMSDE보다 2D MVXD iMSDE를
사용하는 것이 보다 진단적 가치가 높은 영상을 얻을 수 있을 것으로 사료된다.





| 1. | 통계청. 2015년 사망원인통계. http://kostat.go.kr/portal/korea/kor_nw/2/1/index.board?bmode. |
|---|---|
| 2. | William S. Kerwin. Carotid artery disease and stroke: assessing risk with vessel wall MRI. ISRN Cardiology, 2012;article ID 180710:13-67. |
| 3. | Huilin Zhao, Jinnan Wang, Xiaosheng Liu, et al. Assessment of carotid artery atherosclerotic disease by using three-dimensional fast black-blood MR imaging: comparison with DSA. Radiology, 2015;274(2):508–516. |
| 4. | Wintermark, S.S. Jawadi, Rapp J.H., et al. High-resolution CT imaging of carotid artery atherosclerotic plaques. American Journal of Neuroradiology, 2008;29(5):875-882. |
| 5. | Duivenvoorden R., de Groot E., Elsen BM, et al. In vivo quantification of carotid artery wall dimensions. Circ Cardiovasc Imaging., 2009;2(3):235-242. |
| 6. | D.R.J. Owen, A.C. Lindsay, R.P. Choudhury, et al. Imaging of atherosclerosis. Annual Review of Medicine, 2011;62:25-40. |
| 7. | Chun Yuan, Minako Oikawa, Zach Miller, et al., MRI of carotid atherosclerosis. J Nucl Cardiol. 2008;15(2):266–275. |
| 8. | Yoshida K., Narumi O., Chin M., et al. Characterization of carotid atherosclerosis and detection of soft plaque with use of black-blood MR imaging. American Journal of Neuroradiology, 2008;29(5):868-874. |
| 9. | Streifler J,Y., Eliasziw M., Fox A,J., et al. Angiographic detection of carotid plaque ulceration : comparison with surgical observations in a multicenter study. North American Symptomatic Carotid Endarterectomy Trial, Stroke, 1994;25:1130–1132. |
| 10. | Wang J., Yarnykh V.L., Yuan C., et al. Enhanced image quality in black-blood MRI using the improved motion-sensitized driven-equilibrium (iMSDE) sequence. J Magn Reson Imaging., 2010;31(5):1256-1263. |
| 11. | Niranjan Balu, Baocheng Chu, Thomas S. Tsukami, et al. Comparison between 2D and 3D high-resolution black-blood techniques for carotid artery wall imaging in clinically significant atherosclerosis. Journal of magnetic resonance imaging, 2008;27:918–924. |
| 12. | Jinnan Wang, Vasily L. Yarnykh, Thomas Hatsukami, et al. Improved suppression of plaque-mimicking artifacts in black-blood carotid atherosclerosis imaging using a multislice motion-sensitized driven-equilibrium (MSDE) turbo spin-echo (TSE) sequence. Magnetic Resonance in Medicine, 2007;58:973–981. |
| 13. | Chengcheng Zhu, Martin J. Graves, Jianmin Yuan, et al. Optimization of improved motion-sensitized driven-equilibrium (iMSDE) blood suppression for carotid artery wall imaging. Journal of Cardiovascular Magnetic Resonance. |
| 14. | Naghavi M., Libby P., Falk E., et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I, Circulation, 2003;108(14):1664-1672. |
| 15. | Boussel L., Herigault G., De La Vega A., et al. Swallowing, arterial pulsation and breathing induce motion artifacts in carotid artery MRI. Journal of Magnetic Resonance Imaging. 2006;23(3):413–414. |
| 16. | Ashish A. Tamhane, Konstantinos Arfanakis, Motion correction in propeller and turboprop-MRI. Magn Reson Med., 2009;62(1):174–182. |
| 17. | Norihide Takaya, Chun Yuan, Baocheng Chu, et al. Association between carotid plaque characteristics and subsequent ischemic cerebrovascular events stroke. Epub., 2006;37(3):818-823. |
| 18. | Boussel L., Arora S., Rapp J., et al. Atherosclerotic plaque progression in carotid arteries: monitoring with high-spatial-resolution MR imaging-multicenter trial. Radiology, 2009;252(3):789–796. |
| 19. | Crowe L.A., Keegan J., Gatehouse P.D., et al. 3D volume-selective turbo spin echo for carotid artery wall imaging with navigator detection of swallowing. J Magn Reson Imaging., 2005;22(4):583-588. |
| 20. | Masami Yoneyama, Masanobu Nakamura, Makoto Obara, et al. Hyperecho propeller-MRI: application to rapid high-resolution motion-intensive T2 weighted black-blood imaging of the carotid artery vessel wall and plaque. J Magn Reson Imaging., 2017;45(2):515-524. |
| 21. | Young Jun Choi, Seung Chai Jung, Deok Hee Lee, et al. Vessel wall imaging of the intracranial and cervical carotid arteries. Journal of Stroke, 2015;17(3):238-255. |